Gastric phytobezoars as a cause of vomiting in dogs
Dogs eat grass…obviously. Most of the time it seems to go through OK. or sometimes it gets vomited back up. Grass in the gut is an everyday sonographic finding in canine patients and can sometimes present a diagnostic challenge. However, in the vast majority of cases, once identified, it’s usually a fair assumption that it’s an incidental finding rather than the cause of gastrointestinal signs. Usually.
And yet, in 30 years or so I’ve now seen about 10 dogs whose vomiting persisted until gastric ‘grass ball’ phytobezoars were removed surgically or per endoscope and then resolved. As far as I’m aware this is not well-documented in the literature (although to be fair most vets aren’t surprised that it happens).
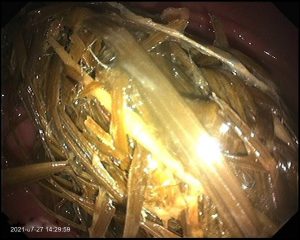
Endoscopic view of a large, stomach-filling grass phytobezoar in a Springer Spaniel

Another angle on the same grass ball. We ended up removing this per endoscope blade by blade. The patient subsequently recovered from what had been a quite debilitating period of hyporexia and vomition.
So, it’s important to be aware that most grass in the stomach is incidental….but there’s always a possibility that it might be a problem in itself if there’s an accumulation. Sonographically, I’ve found gastric phytobezoars challenging.
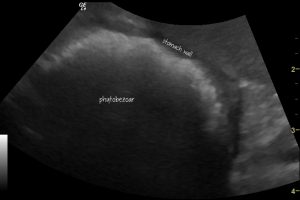
Oblique left-sided view of the gastric fundus and the grass ball within. Although it has a strong shadow suggestive of foreign material, the surface contour is irregular and doesn’t stand out as clearly as, for example, a ball, stone or bone. The same kind of problem is encountered with socks and other fabric FBs. Where the bezoar is up against the gastric wall it’s difficult to be sure that this is foreign material.
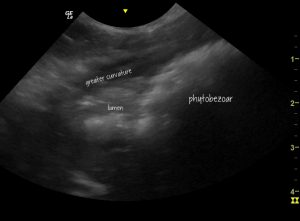
Transverse view of the gastric body (to right of image) and pyloric antrum (to left of image). In this view it’s possible to see the surface of the grass ball diverging from the mucosa. This is the key to identifying foreign bodies with irregular surfaces. The shadowing phytobezoar can be distinguished from the normal stomach content in the lumen towards the pylorus.

Transverse plane view of the pyloric antrum after removal of the bezoar. There’s diffuse hyperechoic change presumably reflecting gastritis due to mechanical abrasion.




Excelente caso clínico
My labrador got a hold of a kids cupcake on Easter, that I later found out I had a party favor plastic ring in the top of it. I didn’t know he had ingested a plastic toy, but I did notice that he was eating grass, which I figured because his stomach was upset. He continued to eat grass for several months, although he behaved and normally otherwise. A little over three months after the Easter party, we were walking in the yard and he all of a sudden started to bear down to vomit. In a pretty swift and easy motion, he vomited up a tightly wound ball of grass about the size of a tennis ball! I dissected it out of curiosity, and directly in the middle, encased in the grass was the plastic Easter ring!